
If you’re running a telemedicine platform or home health marketplace, revenue cycle management in healthcare means something different for you than it does for a hospital billing department. You’re not collecting from payers. You’re disbursing to thousands of providers who expect the same payout speed they’d get from a gig platform. Your ops team might be processing payments just fine at 500 providers, but when you hit 2,000, those manual workflows break fast and provider churn starts before you notice the pattern.
TLDR:
- Healthcare marketplaces handle provider payouts, not patient billing – slow disbursements cost retention.
- Manual provider payments don’t scale past 500 payees without multiplying errors and headcount.
- API-first payout infrastructure triggers disbursements when sessions complete, eliminating ops bottlenecks.
- Routable automates provider payouts across 220+ countries with automated tax compliance and real-time ERP sync.
Understanding Healthcare Revenue Cycle Management in the Marketplace Economy
Most conversations about revenue cycle management in healthcare focus on billing departments chasing down insurance reimbursements. That’s the traditional model, and it’s a different problem from what healthcare marketplace operators actually deal with.
Telemedicine platforms, locum tenens staffing networks, and home health marketplaces don’t struggle to collect money from payers. Their RCM challenge runs the other direction: getting money out accurately and fast to thousands of providers, nurses, and caregivers across their network. The US healthcare RCM market is valued at over $72 billion, and a growing slice belongs to tech-first platforms where provider payout velocity, compliance at scale, and payee experience are the metrics that matter.
Seven Critical Revenue Cycle Stages for Healthcare Marketplaces
The traditional RCM cycle was built around patients and payers. For healthcare marketplace operators, the same seven stages exist but map to a completely different workflow.
Each stage compounds on the last. A credentialing gap in stage two creates a payout error in stage five. A reconciliation failure in stage seven means your finance team is chasing ghosts at month-end.
Why Provider Payment Speed Drives Healthcare Marketplace Retention
Provider churn in healthcare marketplaces rarely traces back to one dramatic moment. It accumulates through late payments, unpredictable deposit timing, and the frustration of chasing down what you’re owed. For nurses, caregivers, and telehealth providers working across multiple platforms, the one that pays fastest and most reliably wins their availability.
73% of workers prefer employers who offer faster access to earnings. In a market where providers can list on three competing platforms simultaneously, payout speed functions as a retention lever.
Locum tenens networks and on-demand caregiving marketplaces fight over the same pool of credentialed providers. If your disbursement cycle runs weekly while a competitor runs same-day ACH, that gap shows up in fill rates before it shows up in your churn report. Speed matters, but predictability matters just as much. Providers want to know when funds arrive, and that the timing stays consistent.
Tax Compliance at Scale for Healthcare Provider Networks
The answer is collecting tax forms at onboarding, not retroactively. Scaling a healthcare provider network past 100 payees turns tax compliance into a year-round risk, as every provider you add requires either a W-8 or a W-9. When onboarding happens fast, manual form collection often falls through the cracks, exposing gaps during audits or causing you to miss 1099-NEC and 1042-S filing deadlines.
By capturing tax data upfront, TIN validation against IRS records runs in the background and flags mismatches before they become filing errors. This prevents the backlog of incomplete records and allows your platform to scale without facing year-end scrambles.
API-First Provider Payout Infrastructure for Healthcare Platforms
Traditional bill pay software wasn’t designed to fire a payment the moment a telehealth session ends. Healthcare marketplace operators need infrastructure that connects care delivery directly to disbursement, without a human manually queuing the run.
An API-first payout layer lets your platform trigger provider payments programmatically based on completed events: a shift logged, a session marked complete, a credentialing check cleared. No ops bottleneck in between.
A few capabilities to look for in any payout API:
- Real-time payment status so providers can track exactly when funds arrive
- Idempotency key support to prevent duplicate payments during retries
- Webhook events that notify your system when a payment clears or fails
- Support for ACH, RTP, and checks without separate integrations per rail
At volume, the difference between polling a dashboard and receiving an automated webhook notification is the difference between a two-person ops team and a six-person one.
White-Label Provider Onboarding and the Payee Experience
When a nurse or telehealth provider joins your network, the first friction point is onboarding. If the bank collection form looks generic or unbranded, trust erodes before the first payment clears.
White-label onboarding lets providers submit payment details inside a branded experience that looks and feels like your product. That consistency matters when you’re asking someone to hand over banking information. A healthcare marketplace competing for the same credentialed provider pool as three other networks wins partial battles through trust signals that competitors overlook.
Self-service payment method selection reduces the support load on your ops team. Providers choose ACH, check, or another available rail on their own schedule, 24/7, without a ticket queue. When providers can see exactly when funds will arrive, the “where’s my payment?” inquiry largely disappears.
ERP Integration Requirements for Healthcare Marketplace Finance Teams
Finance teams running NetSuite, Sage Intacct, or QuickBooks face a specific problem: provider disbursements live in one system while the general ledger lives in another. Without real-time sync between them, reconciliation becomes a manual job that scales badly.
Bi-directional ERP sync means every provider payout posts to the correct entity, cost center, and currency in your ledger automatically. ACH IDs, check numbers, and SWIFT references sync to reference fields so your team can trace any payment without digging through bank statements.
For international provider networks, multi-currency sync matters separately. Payments recorded in the provider’s local currency sync to your base currency without manual conversion entries, removing an entire category of month-end adjustments.
Cross-Border Provider Payments for Global Healthcare Networks
Paying a locum tenens physician in Germany or a remote clinician in Southeast Asia involves local rail requirements, currency conversion, and regional banking rules that vary enough to cause outright rejections in certain corridors.
When geopolitical disruptions block standard channels, healthcare marketplaces need a partner who can manually intercede and route around the blockage. Coverage across 220+ countries matters less than what actually happens when a specific payment corridor goes dark and providers are waiting to get paid.
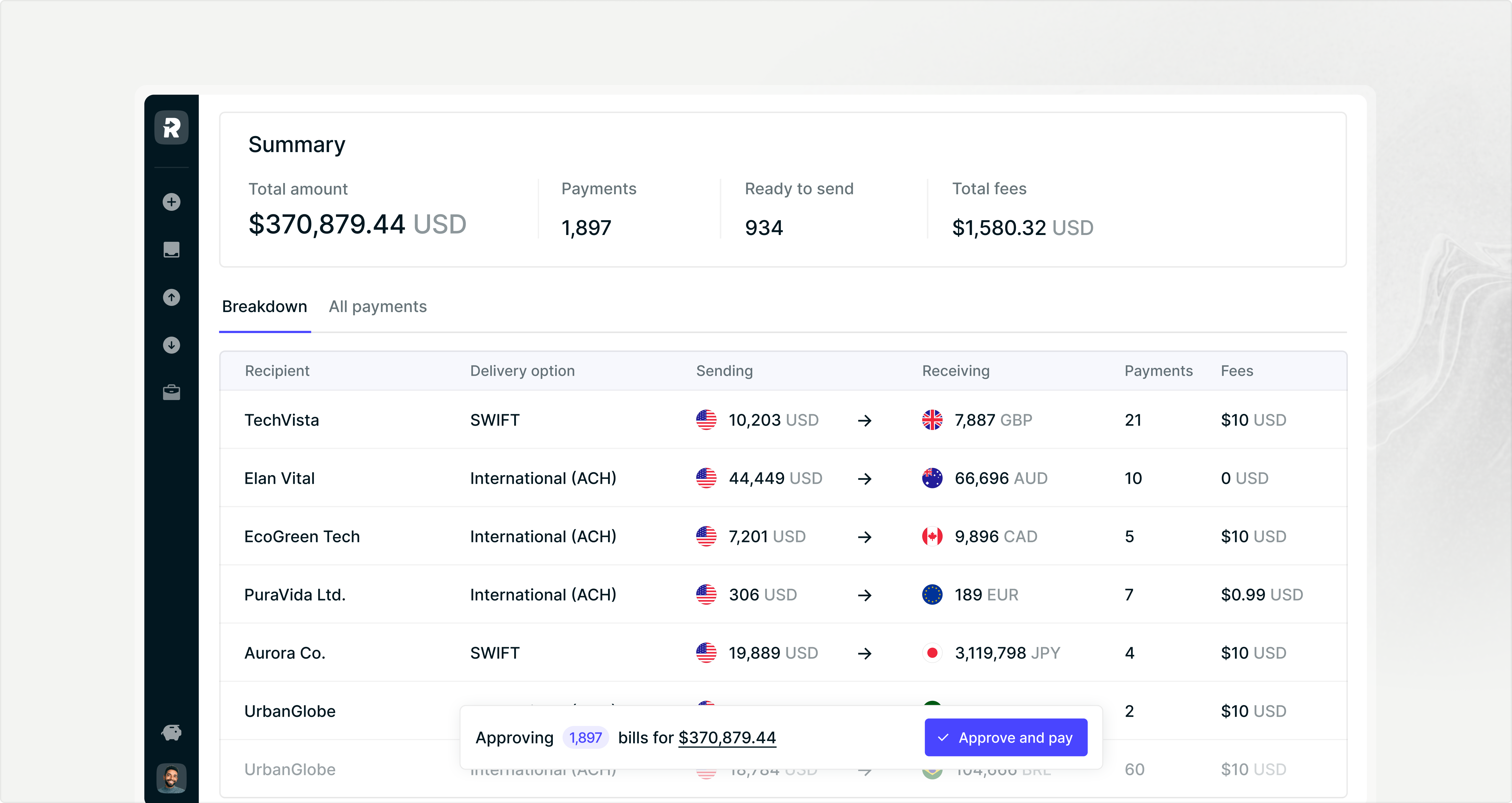
Automating Provider Payouts to Scale Healthcare Marketplace Operations
Triggering provider disbursements through an API the moment a shift closes or a session completes takes the manual queue out of the equation entirely. Routable supports that flow alongside bulk CSV uploads for finance teams who prefer batch runs, with ACH, RTP, checks, and international rails across handled from one system.
W-8, W-9, and TIN validation run during onboarding. Year-end 1042-S, 1099-NEC, and 1099-MISC generation follows automatically from clean records without deadline scrambles.
Bi-directional sync with NetSuite, Sage Intacct, QuickBooks, or Xero posts every payout to the correct entity in real time, scaling from 100 to 10,000+ monthly disbursements without added headcount.
Final Thoughts on Revenue Cycle Management for Healthcare Provider Networks
The traditional revenue cycle management healthcare model was never designed for marketplaces disbursing to thousands of providers who expect payment speed that matches Uber or DoorDash. When your network scales from 300 to 3,000 credentialed professionals, manual CSV uploads and bank portal logins become the bottleneck that costs you fill rates and provider retention. Tax compliance, multi-entity reconciliation, and cross-border payments should all run without your finance team tripling in size.
If you want to see how API-driven provider payouts handle real-time disbursements across ACH, RTP, and international rails, request a demo. The infrastructure that wins in healthcare marketplaces treats payout velocity as a product feature, part of the core experience providers expect.
FAQ
How do healthcare marketplaces automate provider payouts at scale?
Healthcare marketplace operators connect their platform directly to payment infrastructure through API integration or bulk CSV uploads, triggering disbursements programmatically when work periods complete or sessions end. This removes manual payment queuing and scales from hundreds to thousands of providers without adding operations staff.
What payment methods work best for retaining healthcare providers?
Same-day ACH and real-time payments win provider loyalty in competitive healthcare networks, where credentialed professionals often work across multiple platforms simultaneously. Providers consistently choose platforms that pay fastest and offer transparent tracking over those with unpredictable deposit timing.
When should a healthcare marketplace move away from manual provider disbursements?
If your operations team processes more than 300 provider payments per cycle through spreadsheets and bank portals, manual workflows become a scaling liability. Growing provider networks multiply error rates, reconciliation backlogs, and month-end close times that compound with each new provider added.
How do tax forms get collected from hundreds of healthcare providers?
Automated tax form collection during provider onboarding captures W-8 and W-9 forms before the first payment processes, with TIN validation running against IRS records in the background. This prevents year-end filing scrambles and audit documentation gaps that show up when forms are collected retroactively.
What breaks first when healthcare marketplaces scale internationally?
Cross-border provider payments fail when local banking rails, currency conversion requirements, and regional compliance rules vary by corridor. Coverage across multiple countries matters less than having a payment partner who can manually route around geopolitical disruptions when specific payment corridors go dark and providers are waiting to get paid.


